What started with mozzarella sticks, orange chicken, and a giant chocolate chip cookie from Applebee’s changed the course of my life.
I was 17 years old, touring colleges with my parents and preparing for what I thought would be the next exciting chapter of my life when everything changed.
It started with bloody stools and abdominal cramping. At first, my symptoms were dismissed as hemorrhoids. During that time, after taking antibiotics for cystic hormonal acne, I developed C. difficile. Even after treatment, my symptoms persisted for weeks, and two months later a colonoscopy finally provided the answer: ulcerative colitis.
I was a senior in high school.

Senior Prom (2010): Weeks after my first surgery, I attended prom with my ileostomy.
Instead of worrying about prom, graduation, and college, I found myself navigating doctor’s appointments, medications, hospitalizations, and the uncertainty that comes with living with a chronic invisible illness. Over the next year, ulcerative colitis slowly stole pieces of my life. I was exhausted, constantly sick, and missing out on experiences that most teenagers take for granted. I kept wondering, “How can anyone live a normal life with this disease?” As my illness progressed, so did my fears. I found myself wondering if I would need surgery, whether anyone would notice my ostomy, if anyone would ever love me, and if life would ever feel normal again. At 17 years old, I wasn’t just grieving my health – I was grieving the future I thought I was going to have.
Throughout my illness and recovery, my parents – especially my mom – never stopped believing I would get my life back, even during the moments when I couldn’t believe it myself.
Eventually, after a year-long ulcerative colitis flare, my gastroenterologist referred me to a colorectal surgeon. I expected another consultation, another conversation about treatment options. Instead, after examining me that day, he told me my colon was too diseased to save and that I needed surgery. Just one week later, I was in the operating room. I had spent more than a year fighting to keep my colon, hoping each new medication would be the one that finally worked. Accepting surgery didn’t feel like a choice; it felt like admitting defeat. But my body had reached a point where there were no other options. What I couldn’t see then was that surgery wasn’t the end of my life as I knew it. It was my chance to get it back.
At 18 years old, I underwent the first stage of a planned three-stage J-pouch (IPAA) surgery. I woke up with an ileostomy, suddenly trying to make sense of a body that looked and functioned differently than it had before. I couldn’t imagine it then, but the surgery I had fought so hard to avoid would become the beginning of my recovery.
Something unexpected happened almost immediately. For the first time in over a year, I wasn’t running to the bathroom. The urgency and frequency were gone. Even though I had just undergone major surgery, I felt better than I had in months. It was only then that I realized how sick I had truly been.

High School Graduation (2010): Graduating with my ileostomy just two months after undergoing major surgery.
I won’t pretend it was easy. Living with an ostomy at 18 brought fears I never imagined I’d face. Like many young people facing ostomy surgery, I was scared. I worried about how I looked, what other people would think, and whether I would ever feel normal again. Going back to high school with an ostomy felt almost as intimidating as the surgery itself. I wasn’t worried about classes – I was worried about using the bathroom, whether my ostomy would make noise, whether anyone would notice my pouch, and whether I would ever feel like a normal teenager again.
One of the most meaningful moments during that time occurred when a nurse arranged for me to meet another young woman living with an ostomy. Until that moment, I thought my future had been taken from me. Watching her laugh, smile, and live her life changed everything. For the first time, I could picture a future for myself. What I didn’t realize then was that this single act would shape the rest of my life.
From that day forward, little by little, I made a decision: I wasn’t going to let my ostomy stop me from living my life.
I returned to high school. I graduated with my class. I went to my senior prom. I started college. I dated. I wore a bikini. I continued lifeguarding and teaching swim lessons, worked at a boutique shoe store, and even posed for a photoshoot.
None of those moments happened because I stopped being afraid. They happened because I refused to let fear make my decisions.
Looking back, I realized my ostomy wasn’t taking my life away – it was giving it back.
During my first hospitalization, something happened that I never expected. The nurses who cared for me inspired me to become a nurse. Their compassion, patience, and encouragement showed me what it meant to care for someone during one of the most vulnerable moments of life. They didn’t just help me recover, they changed the trajectory of my life. While I was still in the hospital, I knew I wanted to become a nurse. I also knew that one day I wanted to care for patients facing the same fears and life-changing surgeries that I was experiencing. That dream guided every step of my career. I earned my Bachelor of Science in Nursing (BSN), became a Registered Nurse (RN), later completed my Master of Science (MSN) in Nursing as an Adult-Gerontology Acute Care Nurse Practitioner (AGACNP-BC), and ultimately achieved board certification as an Advanced Practice Wound, Ostomy, and Continence Nurse (CWOCN-AP) – the very field that had once cared for me.
I know what it feels like to believe that no one else understands. And I know how powerful it is when someone says, “I’ve been where you are.”
I didn’t become a Wound, Ostomy, and Continence Nurse despite my experience as a patient. I became one because of it.
Today, I work in colorectal surgery, caring for patients with colon and rectal cancer and other complex colorectal conditions. Many are preparing for life with a permanent ostomy, and I have the privilege of helping them navigate that journey. There’s something uniquely powerful about caring for patients when you’ve been the patient yourself.

Bachelor of Science in Nursing (BSN) Graduation (2015): Earning my BSN and beginning the journey toward becoming the nurse I once needed.
Every day, I care for patients facing many of the same fears, decisions, and questions that once terrified me. I sit beside patients preparing for ostomy surgery. I answer the questions they’re often afraid to ask. Most importantly, I remind them that an ostomy is not the end of their story – it’s the beginning of a new chapter.
Because once upon a time, someone did that for me.
Because I’ve been there.
I know what it feels like to wake up after surgery and wonder what comes next.
I know what it feels like to look in the mirror and see a body that has changed.
I know what it feels like to believe that no one else understands.
And I know how powerful it is when someone says, “I’ve been where you are.”
More than a decade later, those fears didn’t end with me. I still hear the very same questions. With tears in their eyes, patients ask me the same questions I once asked myself:
Will anyone notice?
Will I ever feel normal again?
In that moment, I realize I’m not answering as someone who simply studied ostomy care.
I’m answering as someone who has lived it.
I often tell patients that while I would never have chosen ulcerative colitis, I wouldn’t trade the perspective it has given me. My surgeries didn’t restore the life I had before ulcerative colitis; they gave me a different life – one that still includes challenges, but also purpose, gratitude, and the privilege of helping others navigate the path I once walked.
Looking back, ulcerative colitis changed the trajectory of my life in ways I never could have imagined. If you had told my 18-year-old self that one day I would dedicate my career to caring for ostomy patients, I wouldn’t have believed you.
The disease that once felt like the greatest obstacle in my life ultimately led me to my purpose. It took me years to realize that while ulcerative colitis changed my body forever, it also revealed a calling I never knew I was meant to find. Every time I meet a frightened patient preparing for surgery, I think back to the young woman who met with me all those years ago.

Living Life with a J-pouch: Sixteen years later, traveling the world and proving that life after ulcerative colitis surgery can be full of adventure.
She probably had no idea how much that conversation would shape my life. For years, I kept my story mostly private, sharing it only when I thought it might help a patient. Sixteen years later, I’m sharing it publicly for the same reason someone once shared theirs with me: because sometimes, all it takes is seeing someone who’s been there to believe you’ll be okay.
I hope that by sharing my story, I can be that person for someone else.
Because sometimes the thing that changes your life isn’t the surgery itself.
It’s meeting someone who’s already walked the path you’re about to begin.
It’s realizing you don’t have to face it alone.
It’s realizing your story isn’t ending.
It’s just beginning. ❤️
Kelly Mendello, MSN, AGACNP-BC, CWOCN-AP, OCN, is a Colorectal surgery Nurse Practitioner, Advanced Practice Wound, Ostomy, and Continence Nurse, former ostomy patient, and ostomy advocate. Drawing from both her personal journey and her experience caring for patients with ostomies, she is passionate about patient education, mentorship, and helping others navigate life with confidence after ostomy surgery.
Instagram: @withkellyxo
Email: kellymendellonp@gmail.com















 We went out every day afterward and three days later, I asked her to marry me. She said “Yes but I have to tell you something, I have an ostomy.” Gloria went on to explain that she was diagnosed with ulcerative colitis at six years old. She said that she spent a lot of time worrying about where the bathrooms were, what she ate, etc. her sisters said that she was always in and out of a Children’s Hospital.
We went out every day afterward and three days later, I asked her to marry me. She said “Yes but I have to tell you something, I have an ostomy.” Gloria went on to explain that she was diagnosed with ulcerative colitis at six years old. She said that she spent a lot of time worrying about where the bathrooms were, what she ate, etc. her sisters said that she was always in and out of a Children’s Hospital.




 As you recover, if you have a descending or sigmoid colostomy you may want to ask your doctor or ostomy nurse if you are a candidate for
As you recover, if you have a descending or sigmoid colostomy you may want to ask your doctor or ostomy nurse if you are a candidate for 
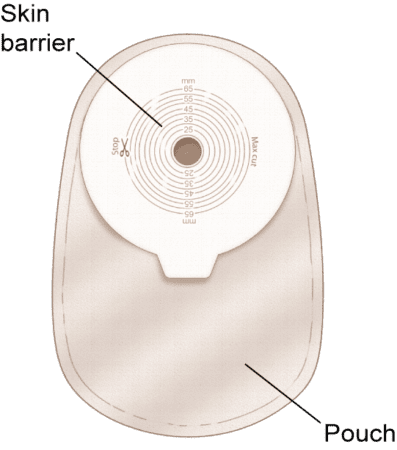
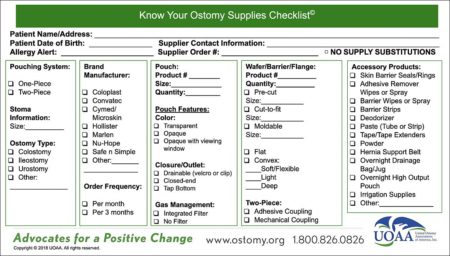
 Picking the best skin barrier is critical since it protects the skin around the stoma and enables a secure seal and fit. Your choice depends on your stoma, output, and other factors, such as sensitivity. Frequent changers may ask about gentle adhesion options while those with liquid output may require a stronger adhesion. If your stoma size is changing or oval you may want to get cut-to-fit or moldable skin barriers while, if it is stable and round, pre-sized are a convenient option.
Picking the best skin barrier is critical since it protects the skin around the stoma and enables a secure seal and fit. Your choice depends on your stoma, output, and other factors, such as sensitivity. Frequent changers may ask about gentle adhesion options while those with liquid output may require a stronger adhesion. If your stoma size is changing or oval you may want to get cut-to-fit or moldable skin barriers while, if it is stable and round, pre-sized are a convenient option.